Understanding psychedelic pharmacology for mental health
TL;DR:
- Understanding psilocybin’s pharmacology reveals that its effects derive from converting into psilocin, which activates serotonin 5-HT2A receptors to induce perceptual and emotional changes. These receptor interactions disrupt neural networks like the default mode network, fostering neuroplasticity and potential long-term mental health benefits. Safe, effective use depends on appropriate set, setting, and awareness of individual contraindications.
Most people who are drawn to psilocybin mushrooms focus on the experience itself: the visuals, the emotional breakthroughs, the sense of connectedness. That’s understandable. But beneath the surface of every meaningful psychedelic journey is a precise biochemical sequence playing out across your brain and body. Understanding that sequence isn’t just for researchers. For anyone in Canada considering psilocybin for mental health, personal growth, or recreational use, knowing the pharmacology behind the effects helps you make better decisions, set realistic expectations, and get the most out of every dose.
Table of Contents
- What is psychedelic pharmacology?
- How psilocybin affects the brain: Chemical pathways and mechanisms
- Therapeutic effects: What the clinical research says
- Risks, contraindications, and best practices for safe use
- New frontiers: Microdosing, whole-mushroom effects, and non-hallucinogenic analogs
- Why intensifying the experience matters more than you think
- Explore psilocybin products and science-based guides
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Psilocybin acts through serotonin | The main benefits stem from activating specific serotonin receptors, especially 5-HT2A. |
| Trip intensity drives outcomes | Research shows the subjective strength of the experience often predicts therapeutic results. |
| Safety depends on context | Risk is much lower with proper screening, preparation, and aftercare, especially in Canada. |
| Microdosing and new analogs | Innovations like microdosing and non-hallucinogenic compounds are shaping the future, but classic subjective effects still matter. |
What is psychedelic pharmacology?
Pharmacology is the science of how drugs interact with biological systems, covering everything from how a substance enters the body to how it changes behavior and mood. When we talk about psychedelic pharmacology, we’re specifically looking at how compounds like psilocybin alter perception, cognition, and emotional processing at a chemical level.
Psilocybin itself is technically a prodrug. That means it doesn’t cause effects on its own. Once you ingest it, your body converts psilocybin into psilocin through a process called dephosphorylation, primarily in the gut and liver. Psilocin is the active compound that actually crosses the blood-brain barrier and starts doing its work.
Here’s a quick breakdown of the core concepts:
- Prodrug: A substance that becomes active only after metabolism inside the body
- Psilocin: The active metabolite of psilocybin, responsible for all psychedelic effects
- Serotonin receptors: The primary targets of psilocin in the brain, especially 5-HT2A
- Agonist: A compound that activates a receptor, mimicking or amplifying natural signals
- Neuroplasticity: The brain’s ability to form new neural connections, believed to underlie therapeutic benefits
As one recent systematic review confirms, psilocybin is rapidly dephosphorylated to psilocin, which acts primarily as an agonist at serotonin 5-HT2A receptors, with additional affinity for 5-HT1A and 5-HT2C receptors.
“The pharmacology of psilocin isn’t a side note to the psychedelic experience. It is the experience. Understanding the receptor targets is what allows researchers and users alike to predict, refine, and build on outcomes.”
This receptor science is why psilocybin’s psilocybin brain effects are so different from those of cannabis or alcohol. It’s not random stimulation. It’s a targeted interaction with one of the brain’s most sophisticated signaling systems.
How psilocybin affects the brain: Chemical pathways and mechanisms
Let’s trace what actually happens from the moment you ingest a dose of psilocybin mushrooms to the point where your perception begins to shift.
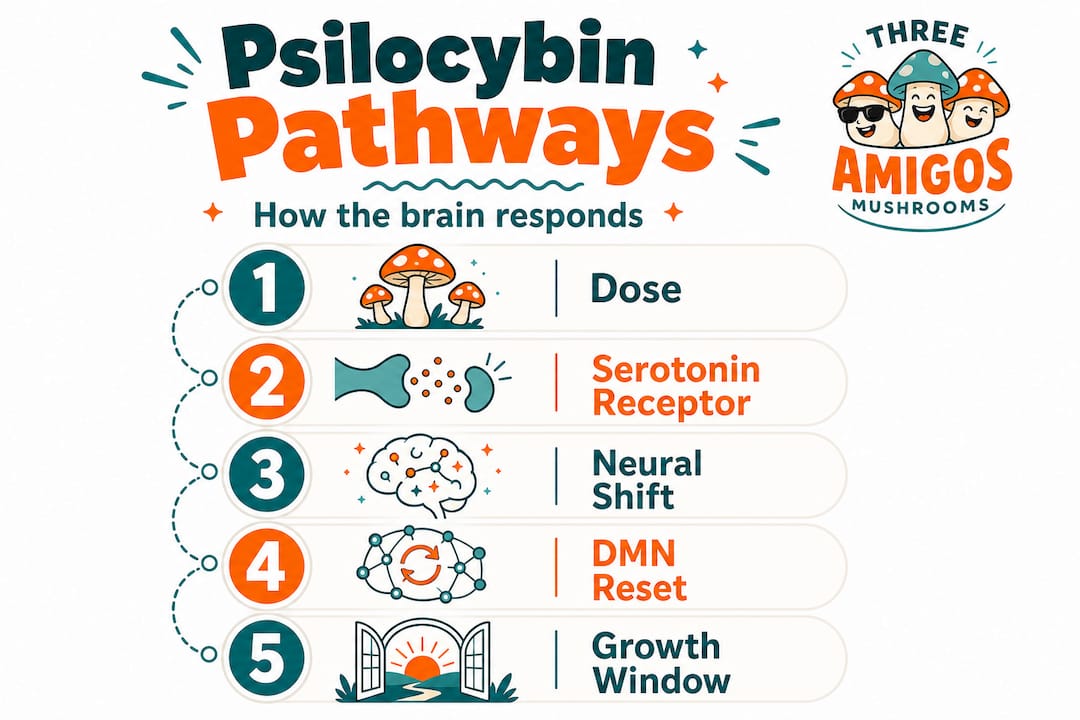
Step-by-step: Psilocybin’s journey through the body
- Ingestion: You eat dried mushrooms, a capsule, or an edible. Psilocybin enters the digestive system.
- Conversion: Enzymes in the gut and liver convert psilocybin to psilocin within 20-60 minutes.
- Absorption and peak: Oral psilocybin absorption reaches peak blood concentration (Tmax) around 2 hours, with levels scaling up depending on dose (dose-dependent Cmax).
- Receptor activation: Psilocin binds primarily to 5-HT2A receptors concentrated in the cortex, hippocampus, and frontal regions.
- Neural disruption and reorganization: Normal brain communication patterns break down temporarily, allowing new connections to form.
- Metabolism: The liver enzymes CYP2D6 (primary), CYP3A4, MAO-A, and UGTs metabolize psilocin, with byproducts excreted mainly through urine.
- Return to baseline: Most effects resolve within 4-6 hours, though neurological changes can persist for days or weeks.
What makes step 5 so significant is the specific nature of the disruption. Research published in 2026 shows that 5-HT2A activation causes acute neural desynchronization, broadband cortical EEG changes, increased glutamate release, and subacute neuroplasticity including dendritic spine growth and synaptogenesis, particularly in pyramidal neurons (PT type) in the medial frontal cortex.
| Brain change | Timing | Effect |
|---|---|---|
| Neural desynchronization | Acute (during dose) | Altered perception, ego dissolution |
| Broadband EEG changes | Acute (during dose) | Disrupted default mode network |
| Glutamate release | Acute to subacute | Increased synaptic activity |
| Dendritic spine growth | Subacute (24-72 hrs) | Enhanced neuroplasticity |
| Synaptogenesis | Subacute to long-term | Potential lasting mood changes |
The default mode network (DMN), the brain circuit associated with self-referential thinking and rumination, is particularly disrupted. This is believed to be why many people report a loosening of rigid thought patterns and an ability to see their problems from a new angle during and after a session.

Pro Tip: The quality of your neuroplasticity window matters. Research suggests that the 24-72 hours after a session, when synaptogenesis peaks, is an ideal time for integration practices like journaling, therapy, or creative work. What you do in that window can shape the lasting impact.
Exploring the full range of effects and benefits of psilocybin is worth your time if you want to build on this understanding with practical context.
Therapeutic effects: What the clinical research says
The clinical data around psilocybin for mental health has moved fast over the past few years. What once existed only in small pilot studies is now supported by structured phase 2 and phase 3 trials, particularly for treatment-resistant depression (TRD) and major depressive disorder (MDD).
One of the most consistent findings is that the intensity of the subjective experience correlates with clinical outcomes. Patients who report stronger mystical experiences or emotional breakthroughs during a session tend to show greater symptom improvements, and these effects are mediated through 5-HT2A activation, though researchers continue to debate whether Gi or Gq signaling pathways are more responsible.
On the numbers side, recent depression trials using a single 25mg dose with therapy support show meaningful MADRS (Montgomery-Åsberg Depression Rating Scale) reductions. A DMT analog trial reported a mean difference of -7.35 versus placebo, with response rates of approximately 12-17% at 12 weeks in phase 3-like settings. These aren’t massive effects on their own, but in a population where conventional antidepressants have failed, they represent real clinical value.
Key findings from recent clinical research:
- A single guided session can produce effects lasting weeks to months
- Benefits appear dose-dependent, with higher doses generally producing stronger outcomes
- Therapy context (preparation, integration, support) amplifies results significantly
- Baseline mental health status influences both the experience and the outcome
- Set and setting are not just anecdotal factors; they show up in clinical trial design as critical variables
“Psilocybin is not a drug you take and wait. It’s more accurate to call it a catalyst. The therapeutic benefit emerges from the interaction between the pharmacology and the psychological work that surrounds it.”
If you’re researching this for personal use, the psilocybin for mental health guide covers the Canadian context in practical terms, including what current exemptions and supervised programs look like.
Risks, contraindications, and best practices for safe use
Psilocybin has a strong safety profile relative to many substances, but that doesn’t mean it’s risk-free for everyone. The current research is clear that certain populations face meaningful risks that shouldn’t be minimized.
Who should avoid psilocybin:
- Anyone with a personal or family history of psychosis, schizophrenia, or bipolar I disorder
- Individuals with serious cardiovascular conditions, since psilocin causes temporary increases in blood pressure and heart rate
- People taking medications that inhibit CYP2D6 or CYP3A4 enzymes, which can alter how psilocin is metabolized and increase intensity unpredictably
- Those on SSRIs, since these drugs may blunt effects (though they don’t fully block them), and the interaction can be unpredictable
- Anyone in an unstable mental health episode or without adequate support structures
Rare but real risks include HPPD (Hallucinogen Persisting Perception Disorder), a condition where visual disturbances persist long after use, and particularly challenging or destabilizing trip experiences that can cause temporary psychological distress. These outcomes are uncommon but more likely in high-dose, unguided settings.
Pro Tip: Set and setting are not optional extras. The best clinical outcomes in research trials come from guided, prepared sessions with professional integration support. If you’re using psilocybin outside a clinical context, treat preparation and integration as seriously as the dose itself.
Reading up on psilocybin safety in Canada and exploring psychedelic safety are practical starting points. And if you’re navigating the legal landscape, the current state of psilocybin legality in Canada is changing rapidly and worth understanding before you make decisions.
New frontiers: Microdosing, whole-mushroom effects, and non-hallucinogenic analogs
The mainstream conversation about psilocybin has shifted significantly. It’s no longer just about full macrodose journeys. Researchers and users are now exploring microdosing protocols, whole-mushroom formulations, and a new class of compounds designed to produce neuroplasticity without hallucinations.
What the emerging research shows:
- Microdosing (typically 0.1-0.3g of dried mushrooms) is widely practiced for mood, focus, and creativity, but robust clinical evidence is still catching up to anecdotal reports. The most rigorous studies show modest effects at best, with strong placebo responses complicating interpretation.
- Whole mushroom effects may differ from isolated psilocybin due to an entourage effect, where multiple compounds like baeocystin, norbaeocystin, and beta-carbolines interact with each other and potentially enhance therapeutic action through multi-target engagement.
- Non-hallucinogenic analogs are being developed to activate neuroplasticity pathways (specifically 5-HT2A signaling) without producing subjective psychedelic experiences. These are exciting in theory, but current human data is limited, and neuroplasticity appears regionally selective to areas with high 5-HT2A density.
- Clinical efficacy and experience: The evidence consistently links therapeutic gains to the intensity of the subjective experience. This creates a difficult question for analog development: can you get the benefit without the trip?
“The whole mushroom may be more than the sum of its parts. The entourage hypothesis in psychedelics is still speculative, but it raises important questions about whether pharmaceutical-grade isolated psilocybin delivers the same effects as naturally grown mushrooms.”
This question matters to the ethical psychedelic research community in Canada, especially as regulatory frameworks evolve and determine whether whole plant medicines or synthesized analogs become the standard.
Why intensifying the experience matters more than you think
There’s a growing push in both research and popular culture to find ways to access psilocybin’s benefits without the intensity of a full psychedelic experience. Microdosing, non-hallucinogenic analogs, and subliminal dosing protocols are all part of this trend. We get the appeal. The idea of getting therapeutic value without having to face the discomfort, vulnerability, or time commitment of a full session is attractive.
But the evidence consistently pushes back against that framing. The clinical data from human trials repeatedly shows that trip intensity correlates with outcomes. The patients who report the strongest psychological breakthroughs, the clearest mystical experiences, or the most emotionally significant sessions are the ones showing the largest reductions in depression scores at follow-up. Methodological challenges, including the near-impossibility of true blinding in psychedelic RCTs, make this data hard to interpret cleanly, but the directional finding is consistent.
What’s also emerging from recent research is that psilocybin’s benefits for personal development operate on multiple levels simultaneously. There’s the neuroplasticity, yes. But there are also epistemic shifts (how you know what you know), reduced psychological modularity (rigid thought compartments loosening), and something researchers are calling “self-rebooting” where core beliefs about the self get temporarily suspended and can be rebuilt with more flexibility. These are not purely chemical processes. They require the subjective experience to unfold.
This doesn’t mean microdosing is useless. It means its mechanism of action is likely different from full-dose therapy, and expecting the same depth of transformation from a sub-perceptual dose is probably unrealistic. We also want to flag the risk of what some therapists call spiritual bypassing, using psychedelic experiences to feel transformed without doing the psychological work that makes transformation stick. The effects of a 25mg psilocybin dose are well-documented, and they involve confrontation, not just expansion.
At Three Amigos, we believe the future of psychedelic therapy isn’t about making the experience smaller or more convenient. It’s about making it safer, better supported, and more accessible to people who can genuinely benefit.
Explore psilocybin products and science-based guides
Understanding the pharmacology is the foundation. Taking that knowledge into practice is where the real work begins.
At Three Amigos, we offer a carefully curated range of microdosing mushroom capsules for those starting with sub-perceptual protocols, along with dried mushroom products for those exploring fuller experiences. Every product comes with quality assurance built in, so you’re working with consistent, reliable material rather than guessing at potency. Alongside the products, our library of educational guides is designed to build on the science. The psilocybin science explained resource connects pharmacology to practical mental health outcomes, and the psilocybin experience guide walks you through preparation, dosing, and integration step by step.
Frequently asked questions
How long do psilocybin’s effects typically last?
Effects generally set in within 30-60 minutes after ingestion, peak around 2-3 hours (consistent with Tmax data showing peak plasma concentration near 2 hours), and fully resolve within 4-6 hours for most people.
Is it possible to benefit from psilocybin without a “trip”?
Non-hallucinogenic analogs are in development and show promise in preclinical models, but current evidence from human trials still links therapeutic outcomes to the intensity of the subjective psychedelic experience, making the “benefits without the trip” concept an open research question rather than an established fact.
Who should avoid using psychedelics like psilocybin?
People with a personal or family history of psychosis, severe cardiovascular conditions, or those taking medications that affect CYP2D6 or CYP3A4 enzyme activity should avoid psilocybin, as documented contraindications include elevated cardiovascular risks and unpredictable drug interactions.
Does dosage matter more than mindset for therapeutic results?
Both are critical and they interact. Dosage drives the pharmacological intensity, but mindset and setting shape how that intensity is processed and integrated, with current trial data consistently showing that preparation and therapeutic context are as important as the chemical dose itself.
Recommended
- Psychedelic neuroscience: Psilocybin’s brain effects explained
- Therapeutic uses of dried mushrooms: mental health 2026
- Psilocybin for Mental Health: What the Research Says in 2025 | 3 Amigos Mushrooms
- Psilocybin science explained: unlock mental health benefits
Thomas Wrona is a writer, designer, and wellness coach who believes that nature’s wisdom provides an antidote to the stress of modern life. As a former pro athlete, he’s all about staying in motion! When he’s not writing you’ll probably find Thomas outside.